

Dr. Sujith Mathew Issac, MS ( Ortho ), MRCS ( EDIN, UK )
Fellowship in Arthroscopy and Sports medicine
Arthroscopy and Sports medicine Specialist

Rotator cuff tears
ROTATOR CUFF TEARS
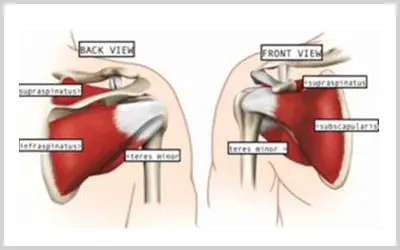
The shoulder joint consists of a ball (humeral head) and socket (glenoid).The main muscles which help to elevate the shoulder are called the rotator cuff muscles. They are four in number : the supraspinatus, infraspinatus, teres minor and the subscapularis.The Supraspinatus is the most commonly torn rotator cuff muscle tendon.
Rotator cuff tears occur mainly in two ways :
- Traumatic : that is after a fall , sudden jerk to the shoulder …etc when the tendon is forcefully torn from the bone
- Degenerative : that is due to wear and tear ; associated with old age or due to friction from an overlying bone ( Impingement from a Sub acromial spur )
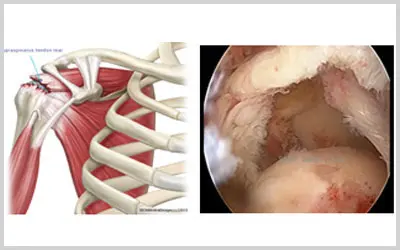
Rotator cuff tear : Diagram (left) & Arthroscopic view (right)
DIAGNOSIS
- Clinical : the main symptom is pain around the shoulder,often radiating down the side of the outer aspect of the upper arm, and often worse at night
- X-Ray : shows changes only in advanced stage when arthritis has set in
- Ultrasound : a good modality in the hands of an expert skeletal sonologist
- MRI : the best modality to assess all parameters of a rotator cuff tear like the diagnosis,number of tendons involved, retraction of the tendon, muscle atrophy, fatty infiltration and other concomitant problems in other parts of the joint.
TREATMENT
Conservative : - includes mainly anti- inflammatory drugs & physiotherapy This may be tried for very small tears and very old patients ( not fit for suregery).In patients with larger tears, some do become relatively pain free with only conservative treatment but this usually lasts only for some time. All studies show that most large tears usually progress over time so that a small tear today becomes a large tear tommorrow and some may deteriorate to the extent that it becomes irreparable.A surgical repair of the tear usually gives good and consistent results provided the condition of the torn muscle and the bone is reasonably good.
SURGICAL REPAIR OF THE ROTATOR CUFF :
We usually do this as a key-hole surgery (arthroscopy). Few tiny holes (3mm) are made around the shoulder for viewing inside the joint and passage of the instruments. First, the tear is assessed and rest of the joint closely inspected to rule out any other problems.Then bone is prepared to enable the tendon to heal to it. Suture Anchors (tiny devices with sutures or “thread” attached) are inserted into the bone and the tendon is repaired to the bone with these sutures.
Arthroscopic Rotator Cuff Repair can be done by different techniques
- Single Row
- Double row (Transs-osseous equivalent or Suture Bridge technique)
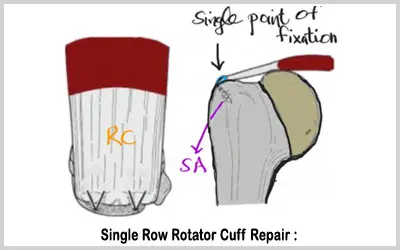
Single Row Rotator Cuff Repair (SR RCR ) :
In this technique, the torn rotator cuff is repaired using a single row of suture anchors
Advantages of SR RCR :
- Easier to perform
- Cheaper
Disadvantages :
- Very high risk of failure of repair (retear rates 20-90%)
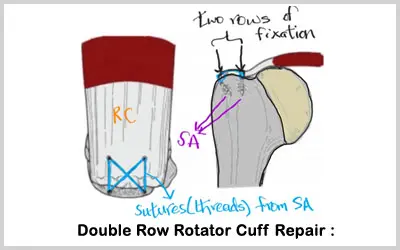
Double Row Rotator Cuff Repair (DR RCR) :
Here, the cuff is repaired using two rows of anchors. It tries to restore the original anatomy of the rotator cuff as closely as possible.This repair is much more secure than a single row repair
Advantages of DR RCR :
- Much more stronger repair construct
- Less chance of failure (retear rates - 10-20%)
Disadvantages of DR RCR :
- a technically more difficult surgery
- costlier ( as more number of Suture Anchors need to be used)
It is to be noted that even with the best techniques, rotator cuff repairs have a failure rate of 10-20%.That is because,the success of the surgery depends on some patient specific factors like :
- the quality of the torn rotator cuff muscle
- the time between the tear and the surgery
( the longer the muscle remains torn,the more it undergoes degeneration , therby affecting the strength of the subsequent repair)
- the tear pattern
- the strength of the bone
But it is encouraging that in our experience, most patients are much better in terms of pain relief as well as shoulder strength after the surgery than before.
See Surgical videos section for a video clip of the procedure
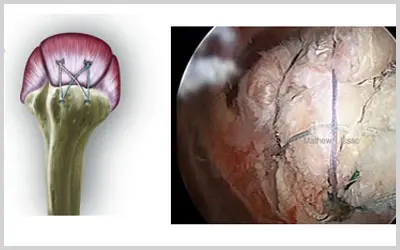
DR RCR : Diagram (left) & Arthroscopic view (right)
POST OPERATIVE REHABILITATION :
- The repaired tendon usually takes 6-12 weeks to heal to the bone. Complete maturation and strengthening of the repair takes around 6 months. The healing time can vary from patient to patient depending on many factors like the quality of the torn rotator cuff tendon , number of tendons torn , and the quality of the bone. After the arthroscopic repair, there will be some pain, varying from a few days to weeks, after which the shoulder should return to normal. A small percentage of patients may develop a “frozen shoulder” – the shoulder is stiff and painful for a few weeks, but this is temporary and always resolves.
- HOSPITAL STAY is short – usually 2 days
- THE OPERATED ARM WILL BE PUT IN A SLING WITH AN ATTACHED PILLOW FOR 6 WEEKS to protect the repair.
- The repaired tendon usually takes 6-12 weeks to heal to the bone. Complete maturation and strengthening of the repair takes around 6 months. The healing time can vary from patient to patient depending on many factors like the quality of the torn rotator cuff tendon , number of tendons torn , and the quality of the bone. After the arthroscopic repair, there will be some pain, varying from a few days to weeks, after which the shoulder should return to normal. A small percentage of patients may develop a “frozen shoulder” – the shoulder is stiff and painful for a few weeks, but this is temporary and always resolves.
- HOSPITAL STAY is short – usually 2 days
- THE OPERATED ARM WILL BE PUT IN A SLING WITH AN ATTACHED PILLOW FOR 6 WEEKS to protect the repair.
- THE SLING IS DISCONTINUED AFTER 6 WEEKS
- FROM 6 WEEKS UNTIL 12 WEEKS, THE OPERATED ARM IS MOVED ONLY WITH THE HELP OF THE OPPOSITE HAND (PASSIVE MOVEMENTS).
- Our physiotherapist will assist you in these excercises, which can be continued at home.
- THE OPERATED ARM IS ALLOWED TO BE ACTIVELY LIFTED (without the help of the opposite hand) ONLY AFTER 12 WEEKS.
- AT THIS STAGE, SPECIFIC EXCERCISES ARE STARTED FOR STRENGHTENING OF THE SHOULDER MUSCLES.
- OUR SPECIFIC EXCERCISE PROTOCOL HAS BEEN DEVISED TAKING INTO ACCOUNT ALL THE MEDICAL EVIDENCE AVAILABLE AT THIS TIME. THIS PROTOCOL IS AIMED AT ALLOWING ADEQUATE TIME FOR THE TENDON TO HEAL TO BONE BEFORE ACTIVELY MOVING THE ARM.
- We are aware that there are many protocols which allow early active movement of the operated arm, but we strongly believe that such over zealous early active movements can jeopardise the repair permenantly. So we go by the dictum “ better safe than sorry”.
EVERYDAY ACTIVITIES AFTER THE SURGERY
FIRST 6 WEEKS
- Daily activies like brushing teeth,shaving,doing hair etc may be difficult, particularly when the dominant shoulder is operated.
- Other activities that also may be difficult are tying shoe laces, hooking up a bra…etc
- Driving is not allowed during this period
- Sleeping on the operated shoulder also may be difficult
6 WEEKS TO 12 WEEKS
- Daily activies like brushing teeth,shaving,doing hair etc may be done without actively lifting the arm.
- Activities that may be difficult are tying shoe laces, hooking up a bra…etc
- Driving is not allowed during this period
- Sleeping on the operated shoulder also may be difficult.
- Working on a computer with the elbow resting on the arm rest is allowed.
AFTER 12 WEEKS
- All routine daily activites like brushing teeth,shaving,doing hair,tying shoelaces..etc can be done.
- Hooking up a bra may still be difficult as that requires extreme rotation of the shoulder.That may be done as the shoulder movement and strength improves gradually.
- Driving is allowed now.
- Heavy lifting and activities which cause sudden jerk to the shoulder are not allowed
SUCCESS RATE
- Atleast 8 out of 10 patients become pain free and have close to or normal function of their shoulders , after the procedure.
- However it has to be emphasized that the post –operative period can be initially painful and dedicated excercises and patience is required.However, the end result after 6 to 8 months is usually very rewarding and satisfying , for both the patient and the surgeon.
- We have reviewed close to a hundred of our patients and have found excellent to good results in 80% of them, moderate in 15% and only 5% had a poor outcome.